Vascular Catheter Preclinical Studies: Animal Models, Endpoints, and Regulatory Pathways
Written by Adir Koreh, CEO of BIOTECH FARM Ltd. and owner of BIOTECH ANATOMY Ltd. — With more than 20 years of hands-on experience in large animal model setup, Adir leads an expert team of veterinarians who have collaborated together for over a decade, delivering scientifically rigorous in vivo results for both industry and academia. This article distills that experience into a practical guide to designing, executing, and submitting vascular catheter preclinical programs that satisfy regulators and protect patients.
Bringing a new vascular catheter from concept to clinic requires a disciplined preclinical strategy that addresses navigation, vessel interaction, hemocompatibility, and long-term tissue response under physiologically realistic conditions. For medical device companies, startups, and CROs working on vascular catheter preclinical programs, the in vivo phase is where bench data meets biology — and where regulators expect rigorous evidence of safety and performance. This article walks through how catheter testing animal models are selected, the endpoints that matter for endovascular device testing, and how to design a catheter safety study that supports timely market access.
???? Expert Insight
The most common and costly mistake in catheter preclinical programs is treating the in vivo study as the first real test of the device. By the time an animal is enrolled, mechanical integrity, biocompatibility, and hemocompatibility must already be characterized. In vivo work answers integrated biological questions that no bench fixture can replicate — and those answers must be earned, not assumed.
Why Animal Models Remain Central to Vascular Catheter Preclinical Evaluation
Bench fixtures and flow loops can characterize mechanical behavior, but they cannot reproduce the dynamic interaction between a catheter and a living vascular bed. Animal studies bridge that gap by exposing the device to pulsatile flow, vessel compliance, coagulation cascades, and inflammatory healing in real time. They are the primary way to surface design issues — kinking under tortuosity, unexpected platelet adhesion, or focal endothelial denudation — before patients are exposed.
The U.S. FDA explicitly outlines when in vivo evaluation is appropriate and what design considerations to apply, framing animal studies as a complement to bench and computational testing rather than a replacement for them. See the FDA guidance on general considerations for animal studies intended to evaluate medical devices for the regulator’s framing.
What Real-World Performance Questions In Vivo Studies Answer
In vivo work allows assessment of trackability through tortuous anatomy, vessel wall trauma during navigation, hemocompatibility under pulsatile flow, and longer-term patency or neointimal response. These attributes determine whether a catheter behaves as intended in patients — not only on a bench.
- Trackability and deliverability through tortuous patient-representative anatomy
- Acute vessel wall trauma including endothelial denudation and dissection
- Hemocompatibility under physiological pulsatile blood flow
- Longer-term patency, neointimal response, and chronic foreign body reaction
Tiered Catheter Device Evaluation: From Bench to Ex Vivo to In Vivo
Catheter device evaluation is rarely a single experiment. It is a progression that builds confidence layer by layer. Bench testing characterizes tensile strength, kink resistance, burst pressure, lubricity, and dimensional accuracy, often informed by FDA guidance on non-clinical engineering tests for intravascular stents and associated delivery systems.
Ex vivo work — isolated tissues, blood loops, simulated circulation — interrogates specific biological interactions such as platelet adhesion or coating elution under controlled conditions. Only then do catheter testing animal models evaluate the integrated device in a living system, where deliverability, deployment, acute injury, and chronic response can be judged together. This staging both reduces risk and reduces unnecessary animal use.
Choosing the Right Animal Model for Vascular Catheter Preclinical Studies

Model selection is driven by the catheter’s intended use, target vessel anatomy, and required follow-up duration. The questions to answer are concrete: Does the species’ vessel diameter and tortuosity match the human target? Are clotting and healing responses translationally relevant? Can the actual procedure be performed with the same imaging and access tools planned for clinical use? A mismatch between catheter geometry and vessel size will distort conclusions about trackability and injury, regardless of how well the rest of the study is run.
Large Animal Models for Endovascular Device Testing
Swine (Pig)
The workhorse for cardiovascular catheters. Coronary, peripheral, and cerebral vasculature closely mirrors human anatomy in size, elasticity, and reactivity — supporting evaluation of deliverability and acute injury under fluoroscopic guidance.
Sheep
Favored for chronic implant studies, especially where tissue ingrowth and sustained patency over months are key endpoints. Excellent tolerance for prolonged follow-up and well-characterized healing biology.
Rabbit
Useful for selected peripheral applications, including intimal hyperplasia and restenosis evaluation. Widely used for balloon-injury restenosis models and early feasibility data.
When Small Animal Models Fit a Catheter Safety Study
Rats and mice are not substitutes for large-animal procedural simulation, but they have a defined role in early-stage screening: coating biocompatibility, localized tissue response, and proof-of-concept for drug-eluting components. They are cheaper, faster, and amenable to genetic tools — but their vessel dimensions and procedural realism are limited. Used wisely, they help filter candidates before committing to large-animal work.
Key Endpoints for Vascular Catheter Preclinical Studies
Endpoints in catheter testing animal models are multifactorial, spanning procedural performance, vascular injury, hemocompatibility, and chronic biology. Procedural endpoints capture deliverability, deployment success, and complication rates such as perforation, dissection, or spasm. Vascular injury endpoints combine angiographic patency assessment with histopathology that quantifies endothelial damage, intimal hyperplasia, and thrombus formation. Hemocompatibility endpoints — thrombus burden, platelet activation, fibrin deposition — are anchored in ISO 10993-4.
How Endpoints Differ Across Acute, Subacute, and Chronic Studies
Acute Studies
Minutes to Hours
Focus on immediate procedural safety, gross vessel injury, deployment success rates, and acute thrombotic events. Fluoroscopy and angiography drive real-time assessment.
Subacute Studies
Days to Weeks
Capture early healing response, short-term patency, and evolving inflammatory reactions. Histopathology reveals initial neointimal formation and early smooth muscle response.
Chronic Studies
Weeks to Months
Evaluate sustained biocompatibility, durability, device integrity over time, mature neointimal formation, foreign body reaction, and long-term efficacy in physiological conditions.
Comparing Bench, Ex Vivo, and In Vivo Testing Layers
Understanding where each testing layer adds value — and where it falls short — is essential for building a program that is both efficient and defensible to regulators.
| Testing Layer | Primary Question | Strengths | Limitations |
|---|---|---|---|
| Bench | Mechanical and dimensional integrity | Reproducible, fast, low cost | No biological response |
| Ex Vivo / Blood Loop | Material–blood interactions | Controlled hemocompatibility readouts | No systemic physiology |
| Small Animal In Vivo | Localized biology, coatings | Cost-effective screening | Anatomical mismatch with humans |
| Large Animal In Vivo | Procedural realism, chronic response | Translational relevance | Higher cost, complex logistics |
How Vascular Injury Is Assessed During Catheter Device Evaluation
Vascular injury assessment combines real-time imaging with post-mortem analysis. Periprocedural fluoroscopy and contrast angiography visualize dissection, perforation, spasm, and thrombus while characterizing flow. Intravascular imaging — OCT and IVUS — adds high-resolution views of vessel wall layers and immediate post-procedural damage. Histopathology then closes the loop, with standardized scoring of endothelial loss, smooth muscle proliferation, inflammation, and neointimal formation in explanted vessels.
The combination is more informative than any single method — and it is what regulators look for when judging whether a device’s interaction with the vessel wall is acceptable for clinical use.
“Histopathology of explanted vessels is the gold standard for characterizing device-induced vascular injury. Angiography shows function; histology reveals mechanism. Both are required for a defensible submission.”
— Adir Koreh, CEO, BIOTECH FARM Ltd.
Evaluating Thrombosis and Hemocompatibility for Catheters

Hemocompatibility is non-negotiable for any blood-contacting catheter. The assessment starts in vitro and ex vivo with blood loops and simulated flow that quantify platelet adhesion, activation, and thrombus formation under controlled shear — following principles described in peer-reviewed hemocompatibility testing literature and broader reviews of in vitro hemocompatibility testing of medical devices.
In vivo work then evaluates thrombus on the catheter surface and at the placement site, monitors systemic coagulation parameters, and uses histopathology of explanted devices and surrounding tissues to characterize burden and reaction. For deeper context on integrating these layers, see the resource on animal studies for medical devices.
✅ Hemocompatibility Endpoint Checklist (ISO 10993-4)
- Platelet adhesion and activation quantification
- Thrombus formation on device surface and vessel wall
- Complement activation and fibrin deposition
- Hemolysis assessment under shear conditions
- Systemic coagulation parameter monitoring in vivo
Feasibility Versus GLP Catheter Safety Study: Knowing the Difference
Feasibility studies are non-GLP, exploratory, and iterative. They optimize technique, refine geometry, and answer “does this work in principle?” with smaller animal numbers and flexible protocols. GLP catheter safety studies, by contrast, are conducted under the OECD Principles on Good Laboratory Practice, with rigorous documentation, quality assurance oversight, and defined animal welfare standards.
Feasibility Study
- Non-GLP, exploratory design
- Smaller animal numbers, flexible protocol
- Iterative — design learning and optimization
- Not for regulatory submission data
GLP Pivotal Study
- Full OECD GLP compliance with QA oversight
- Power-justified animal numbers, locked protocol
- Rigorous documentation and audit trail
- Generates regulator-ready submission data
When a Phased Feasibility-to-GLP Approach Pays Off
Most successful programs run feasibility first to lock the design and procedure, then commit to GLP for the pivotal data package. This sequencing avoids running expensive GLP work on an unfinished device. A practical overview of this stage is available in this discussion of pivotal GLP studies.
Realistic Timelines for Preclinical Catheter Testing
Timelines vary widely. A focused feasibility study can be executed in weeks once protocols and ethics approvals are in place. A chronic GLP study with multi-month follow-up, full histopathology, and statistical analysis typically spans many months. Key drivers include device complexity, follow-up duration, animal numbers, scope of pathology, regulatory documentation requirements, and ethics committee review timelines.
⚠️ Common Timeline Pitfall
Ethics committee review periods are frequently underestimated. In Israel, the Council for Animal Experimentation approval process has defined application windows and review cycles. Sponsors who treat ethics approval as a parallel-path activity — rather than building it into the critical path — routinely push study start dates by months without moving their regulatory milestones. Plan ethics submission before design freeze, not after.
How Many Animals Are Needed for a Catheter Study
Sample size is a balance of statistical power and ethics. Power calculations justify the minimum number needed to detect meaningful differences, while the 3Rs framework — Replacement, Reduction, Refinement — directs teams to minimize use and distress wherever scientifically valid, as detailed in the Guide for the Care and Use of Laboratory Animals.
Smart design choices — using contralateral vessels, including multiple test articles per animal where appropriate, and establishing robust controls — can meaningfully reduce numbers in endovascular device testing without compromising data quality or statistical validity.
Where Non-Animal Alternatives Fit, and Where They Fall Short
Phantoms, bench rigs, and computational fluid dynamics shine for mechanical performance, deliverability, and shear-stress modeling. In vitro assays cover cytotoxicity, genotoxicity, and several hemocompatibility endpoints. None of these replicate integrated healing, foreign body response, or long-term patency under pulsatile flow with active coagulation and immunity.
The most efficient strategy is hybrid: exhaust bench, ex vivo, and in vitro questions first, then use in vivo studies precisely and only where biology is the answer — not as a default starting point.
Mandatory Tests Before Proceeding to In Vivo Catheter Testing
Before any animal is enrolled, a foundation of biocompatibility and mechanical testing must be in place. Biocompatibility follows the ISO 10993-1 framework, with endpoints mapped to device category. For blood-contacting catheters, this means cytotoxicity, sensitization, irritation, hemolysis, complement activation, and thrombogenicity must be characterized.
Mechanical testing — tensile, burst, fatigue, lubricity — must confirm the device meets specification. Skipping these steps risks costly in vivo failures rooted in problems that should have been caught earlier. For program-level context, see this overview of medical device development.
Pre-In Vivo Mandatory Checklist
- ISO 10993-1 biocompatibility risk assessment completed
- Cytotoxicity, sensitization, and irritation confirmed negative
- In vitro hemolysis and hemocompatibility screening complete
- Mechanical specification testing: tensile, burst, kink, lubricity
- Device traceability, sterilization validation, and labeling complete
Common Mistakes in Vascular Catheter Preclinical Programs
Several recurring missteps slow programs down and create costly rework. Each of the following is avoidable with deliberate upfront planning and an experienced team.
Mistake #1
Wrong Species Selection
Choosing a model based on cost rather than anatomical relevance distorts trackability and injury data in ways that cannot be corrected at the reporting stage.
Mistake #2
Skipping Feasibility Phase
Compressing feasibility into the first GLP study locks design errors into an audited, expensive data package that cannot easily be amended.
Mistake #3
Underpowered Chronic Endpoints
Insufficient animal numbers for chronic durability endpoints leave regulators unconvinced about long-term performance and may trigger additional studies.
Mistake #4
Hemocompatibility as a Checkbox
Treating hemocompatibility as a single in vitro test rather than an integrated readout across in vitro, ex vivo, and in vivo phases creates evidence gaps regulators will identify.
Mistake #5
Underestimating Ethics Timelines
Ethics committee review periods are not discretionary. Building them into the critical path from day one — not as a parallel assumption — prevents study start delays from becoming submission delays.
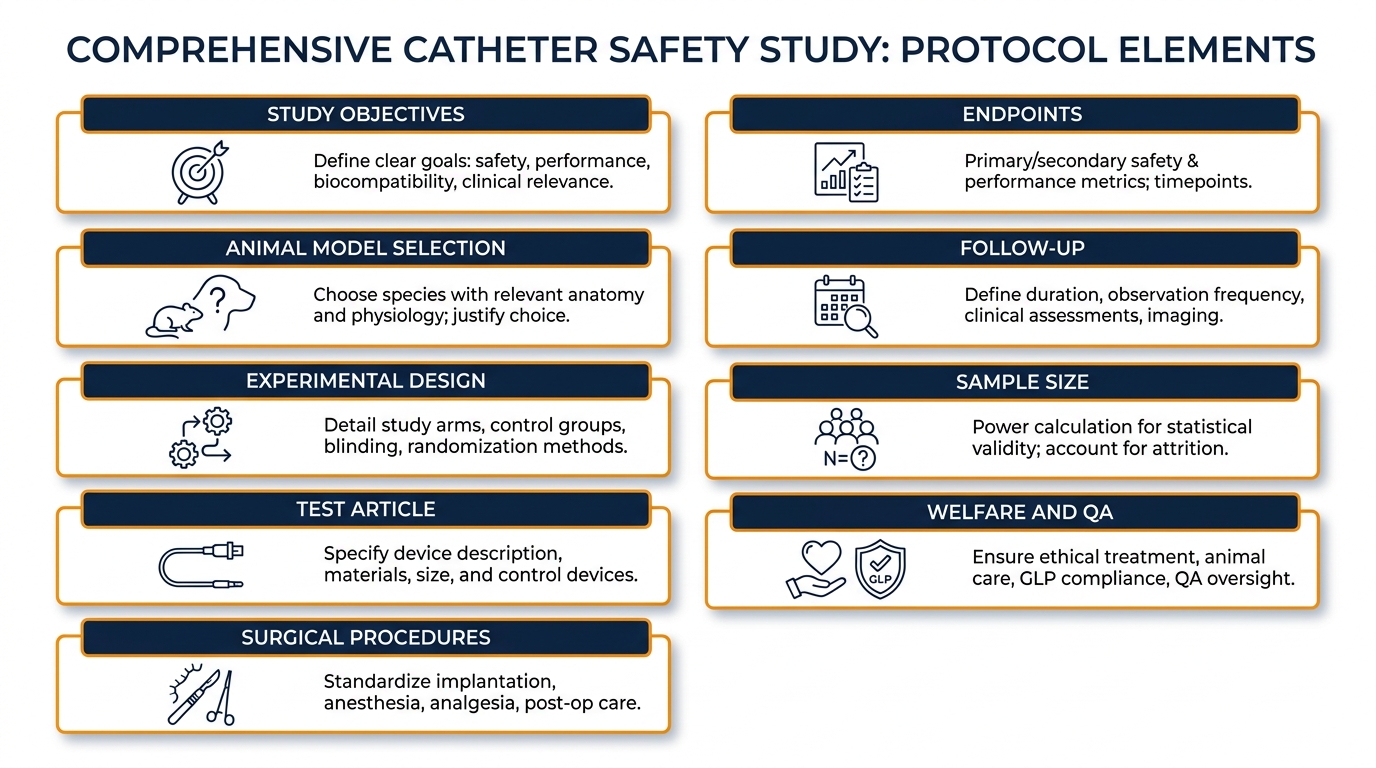
What a Comprehensive Catheter Safety Study Protocol Contains
| Protocol Element | What It Defines |
|---|---|
| Study Objectives | Hypotheses and primary research questions |
| Animal Model Selection | Species, strain, age, sex, and scientific justification |
| Experimental Design | Controls, randomization, and blinding where applicable |
| Test Article | Materials, dimensions, sterilization, and traceability |
| Surgical Procedures | Access, anesthesia, deployment, and imaging protocols |
| Endpoints | Procedural, vascular injury, hemocompatibility, and chronic |
| Follow-up | Acute, subacute, or chronic windows matched to clinical use |
| Sample Size | Power-based justification and 3Rs alignment |
| Welfare and QA | Veterinary oversight, GLP compliance, and audit records |
A protocol that addresses each element — and that is reviewed by all stakeholders before execution — is the backbone of a defensible regulatory submission. Programs aiming for pivotal data should align their quality systems early; this resource on GLP accreditation is a useful reference.
Mapping Business Needs to a Preclinical Partner’s Capabilities
Experienced partners de-risk programs by combining regulatory fluency, surgical expertise, and infrastructure. The table below maps common sponsor needs to what an integrated preclinical facility delivers.
| Business Need | How an Integrated Preclinical Facility Helps |
|---|---|
| Translational anatomy match | Access to large animal models suited to coronary, peripheral, and structural targets |
| Procedural realism | Surgical suites with C-Arm fluoroscopy, high-definition cardiac ultrasound, and 4K laparoscopic towers |
| Regulatory readiness | Protocols designed against FDA, ISO 10993, and OECD GLP expectations |
| Iterative design support | Phased feasibility-to-pivotal pathway with scientific escort throughout |
| Animal welfare and ethics | Documented procedures, transparent collaboration, and a 3Rs-aligned operational culture |
| Local context for Israeli sponsors | Familiarity with Israeli ethics committee processes and a fully managed on-site facility |
“The value of an experienced partner is not just infrastructure — it is the scientific escort that translates regulatory expectations into executable protocols, and executes those protocols with senior surgeons who have done it before.”
— Adir Koreh, CEO, BIOTECH FARM Ltd. & Owner, BIOTECH ANATOMY Ltd.
Frequently Asked Questions
Ready to Plan Your Next Catheter Study?
If you are scoping a vascular catheter preclinical program and weighing model selection, endpoints, or the path from feasibility to pivotal GLP, our team is ready to work through the details with you. What is the single decision that, made well now, would most reduce risk later?