IND vs NDA in Preclinical: Why the Distinction Shapes Your Entire Development Plan
Authored by Adir Koreh, CEO of Biotech Farm Ltd. — 20+ years of large-animal model expertise — and the Biotech Farm scientific team. This in-depth guide breaks down how IND-enabling and NDA preclinical requirements diverge, and what that means for your development timeline and budget.
✔ GLP Toxicology
✔ Large Animal Models
✔ FDA Regulatory Strategy
Sponsors who plan their NDA-stage nonclinical strategy during IND-enabling design avoid the most expensive mistake in drug development: repeating pivotal studies. Species selection, formulation decisions, and toxicology study duration made at the IND stage lock in consequences that echo all the way to label language and post-marketing commitments.
At the heart of medical innovation, preclinical R&D services are pivotal in translating scientific research into potentially life-saving treatments. Yet many sponsors enter the regulatory landscape without a precise understanding of how an Investigational New Drug (IND) submission diverges from a New Drug Application (NDA) — particularly in the nonclinical data they require. The IND vs NDA preclinical differences represent two distinct regulatory milestones, each with its own data scope, study quality expectations, and strategic timing.
An IND seeks permission to administer an investigational drug to humans for the first time, focusing on demonstrating reasonable safety. An NDA, by contrast, is the comprehensive marketing application that integrates preclinical, clinical, and CMC data to demonstrate safety and efficacy for general use. Understanding where these dossiers overlap — and where they sharply diverge — helps sponsors plan resources, design pivotal studies, and avoid costly delays.
What Exactly Is an IND?
An IND is a regulatory submission to the FDA (or equivalent authority) requesting authorization to administer an investigational drug or biologic to humans. Its primary purpose is to ensure the safety of trial participants based on preliminary nonclinical data, chemistry-manufacturing-controls (CMC) information, and clinical protocols.
The IND application includes preclinical (nonclinical) studies demonstrating reasonable safety for initial human exposure, manufacturing and quality information ensuring consistent production, and detailed clinical protocols outlining proposed human studies — including dosages, duration, and monitoring plans.
30-Day Review Clock
Studies may begin 30 days after FDA receives the IND unless a clinical hold is imposed. The IND is permission to investigate — not marketing approval.
Reasonable Safety Standard
The evidentiary bar for an IND is “reasonable safety” — not the comprehensive benefit-risk evidence required for an NDA. The bar scales with clinical risk.
Fit-for-Phase CMC
Manufacturing standards at IND stage need only be sufficient to ensure identity, quality, purity, and strength for the specific proposed clinical trial.
Defining the NDA: The Marketing Authorization Dossier
An NDA is a comprehensive submission requesting approval to market a new drug in the United States. It must demonstrate, through substantial evidence, that the drug is safe and effective for its intended use(s). The NDA integrates all available data from preclinical, clinical, and CMC development to support a complete benefit-risk assessment.
For preclinical stages FDA approval in the NDA context, the nonclinical section (Module 4 of the Common Technical Document) provides a complete characterization of the drug’s nonclinical safety profile. This data supports the eventual drug label, post-marketing safety surveillance commitments, and regulatory decisions about appropriate patient populations, contraindications, and warnings. While the IND opens the door, the NDA closes the development loop with a full evidentiary record.
“The NDA is where years of preclinical and clinical work converge into a single narrative — and any gaps in nonclinical data surface with consequence, from label restrictions to post-marketing study commitments.”
— Adir Koreh, CEO, Biotech Farm Ltd.
When Do You File an IND, and When Should You Start Thinking About the NDA?
An IND is typically filed once sufficient IND-enabling studies are completed to justify initiating human trials — usually before Phase 1. These studies must collectively make the case that the proposed first-in-human dose, regimen, and duration carry acceptable risk. For a deeper dive into these critical preparatory studies, see the guide on Biotech IND-enabling preclinical studies & filing.
Thinking about the NDA, however, begins much earlier — sometimes as early as lead optimization. Decisions made about species selection, formulation, impurity profile, and toxicology study design during the IND-enabling phase often have downstream consequences for the NDA. Sponsors who plan with the end in mind tend to avoid repeating studies, bridging gaps, or facing unexpected label restrictions years later.
Discovery Phase vs IND-Enabling Phase
Target identification, lead generation, and optimization to select a promising drug candidate. Focus is on scientific proof-of-concept, not regulatory formatting.
Regulatory-driven nonclinical studies designed to assess potential risks to humans — including safety pharmacology, GLP toxicology, and PK studies that inform the first-in-human dose and duration.
Side-by-Side: How the Two Submissions Compare

| Dimension | IND | NDA |
|---|---|---|
| Regulatory goal | Permission to start human trials | Permission to market the drug |
| Preclinical scope | Targeted, supports FIH safety | Comprehensive, supports full label |
| Toxicology duration | Matches or exceeds proposed clinical exposure | Includes chronic, carcinogenicity, repro/dev |
| CMC maturity | “Fit-for-phase” | “Commercial-ready” |
| Review clock | 30 days (default effective) | Standard 10 months / Priority 6 months |
| Data evidentiary bar | Reasonable safety | Substantial evidence of safety + efficacy |
Which Preclinical Data Are Mandatory to File an IND?
To file an IND, a core package of nonclinical data is required to establish “reasonable safety” for initial human exposure. This package generally includes pharmacology studies (primary mechanism of action and secondary off-target effects), toxicology studies (acute and repeat-dose in relevant species to identify target organs and a NOAEL), safety pharmacology studies addressing cardiovascular, respiratory, and CNS effects per ICH S7A, and pharmacokinetics/toxicokinetics studies characterizing ADME and exposure-response relationships.
- Primary mechanism of action
- Secondary off-target effects
- Acute and repeat-dose tox in two species
- NOAEL determination
- Cardiovascular effects
- Respiratory and CNS effects
The extent and duration of these studies depend on the proposed clinical trial design — single ascending dose vs multiple ascending dose, healthy volunteers vs patients, and short-term vs long-term exposure. Bridging the gap between laboratory discoveries and clinical trials requires precision in study design, with each nonclinical endpoint mapped back to a specific clinical question.
What “Really Counts” as IND-Enabling — A Category-Level Checklist
IND-enabling studies are nonclinical studies specifically designed and conducted to support the safety of initiating human clinical trials. They are characterized by regulatory focus, quality standards (often GLP-compliant for pivotal toxicology), and formal reporting suitable for regulatory submission. What truly counts as IND-enabling are studies whose outcomes directly inform the initial human dose, duration, and safety monitoring plan.
| Category | Typical Expectation |
|---|---|
| Primary Pharmacology | Mechanism of action, relevance to human disease |
| Secondary Pharmacology | Off-target effects, binding profiles |
| Safety Pharmacology Core Battery | CV, CNS, respiratory (per ICH S7A) |
| Repeat-Dose Toxicology | Two species (one non-rodent), duration ≥ clinical exposure |
| Toxicokinetics | Exposure correlation with toxicity |
| Genotoxicity | Ames, chromosomal aberration / micronucleus |
| CMC Readiness | Fit-for-phase manufacturing and stability |
Does Every Preclinical Study Have to Be GLP to Support an IND?
Not all preclinical studies for an IND require adherence to Good Laboratory Practice regulations. Pivotal toxicology studies — particularly repeat-dose studies that determine the NOAEL and inform the maximum recommended starting dose (MRSD) in humans — are generally expected to be GLP-compliant. Non-GLP studies, such as early pharmacology or some ADME work, are acceptable when they are scientifically sound and provide reliable supporting data.
For an NDA, regulatory agencies expect most nonclinical studies critical to the safety assessment to be GLP-compliant or adequately justified if not, per 21 CFR 314.101. Conducting well documented procedures under recognized quality systems — combined with transparency in collaboration between sponsor and CRO — is what allows nonclinical data to withstand regulatory scrutiny across both submissions.
- Pivotal repeat-dose toxicology
- Safety pharmacology core battery
- Studies that determine NOAEL / MRSD
- Early exploratory pharmacology
- Exploratory ADME studies
- Proof-of-concept efficacy work
Preclinical Package for IND vs Preclinical Package for NDA: A Practical Difference
The preclinical package for an IND is designed to support the safety of initial human exposure, focusing on acute and subacute toxicity and risks specific to the proposed clinical trial. The preclinical package for an NDA is far more comprehensive — aiming to fully characterize the drug’s safety profile over its entire anticipated clinical use, including chronic exposure, carcinogenicity potential, reproductive and developmental toxicity, and specific target organ toxicities.
A Concrete Illustration
“Is the candidate safe enough for a 7-day single or multiple ascending dose study in healthy volunteers?”
“What are the long-term toxicities in patients? Are there reproductive risks? Is it carcinogenic after years of use? How do drug-drug interactions impact safety in real-world populations?”
The preclinical stages form a continuous process supporting drug development from discovery through marketing approval, articulated in ICH M3(R2), which sets out international expectations for the timing and scope of nonclinical safety studies relative to clinical development.
How Sponsors Translate Preclinical Data into a Safe First-in-Human Dose
Determining the safe first-in-human (FIH) dose is one of the most consequential outputs of IND-enabling studies. The FDA approach typically involves identifying the NOAEL in the most relevant animal species, converting to a Human Equivalent Dose (HED) using body surface area scaling, applying a default safety factor (often 10x), and adjusting based on pharmacological activity, exposure margins, and the most sensitive species.
- Inadequate species selection — using species not relevant to human toxicology
- Insufficient exposure in animal studies relative to anticipated human levels
- Poor PK correlation between species leading to dose miscalculation
- Overlooking safety pharmacology signals that were present but under-reported
Preclinical Causes of Clinical Hold: What Triggers FDA Concern?

A clinical hold is an order issued by the FDA to delay a proposed clinical investigation or suspend an ongoing one, defined under 21 CFR 312.42. Preclinical deficiencies are among the most common reasons. Typical triggers include:
- Unreasonable risk to subjects from unacceptable toxicity or insufficient safety margins
- Deficient or incomplete nonclinical information in the submission
- Poor study quality where data cannot be relied upon
- Inadequate justification for the starting dose or escalation scheme
- Mismatch between preclinical findings and the clinical monitoring plan
Preventing a clinical hold begins long before submission — it begins with rigorous study design, qualified species, adequate exposure characterization, and a coherent narrative connecting nonclinical observations to clinical risk mitigation. Working with a scientifically supportive services provider helps sponsors anticipate FDA concerns and address them proactively.
CMC at the Preclinical Stage: IND vs NDA Expectations
For an IND, the CMC section needs to be “fit-for-phase,” providing sufficient information to assure identity, quality, purity, and strength of the investigational product for the proposed clinical trial. This generally includes a description of drug substance and drug product, manufacturing process, analytical methods, and stability data covering the trial duration.
For an NDA, the CMC section must be “commercial-ready” — full details on validated manufacturing processes for both drug substance and drug product, detailed specifications, validated analytical methods, long-term stability data supporting expiry dating, and a robust quality system for global supply. Preclinical work often informs CMC by identifying impurities or degradation products with toxicological relevance.
???? Fit-for-Phase (IND)
Sufficient data to ensure the investigational product is safe and consistent for early clinical investigation. The manufacturing process may still evolve as development progresses.
???? Commercial-Ready (NDA)
Complete data demonstrating the manufacturing process is fully controlled, stable, and scalable to consistently produce a high-quality product for wide commercial distribution.
Where a Specialized Large-Animal Preclinical Partner Adds Value
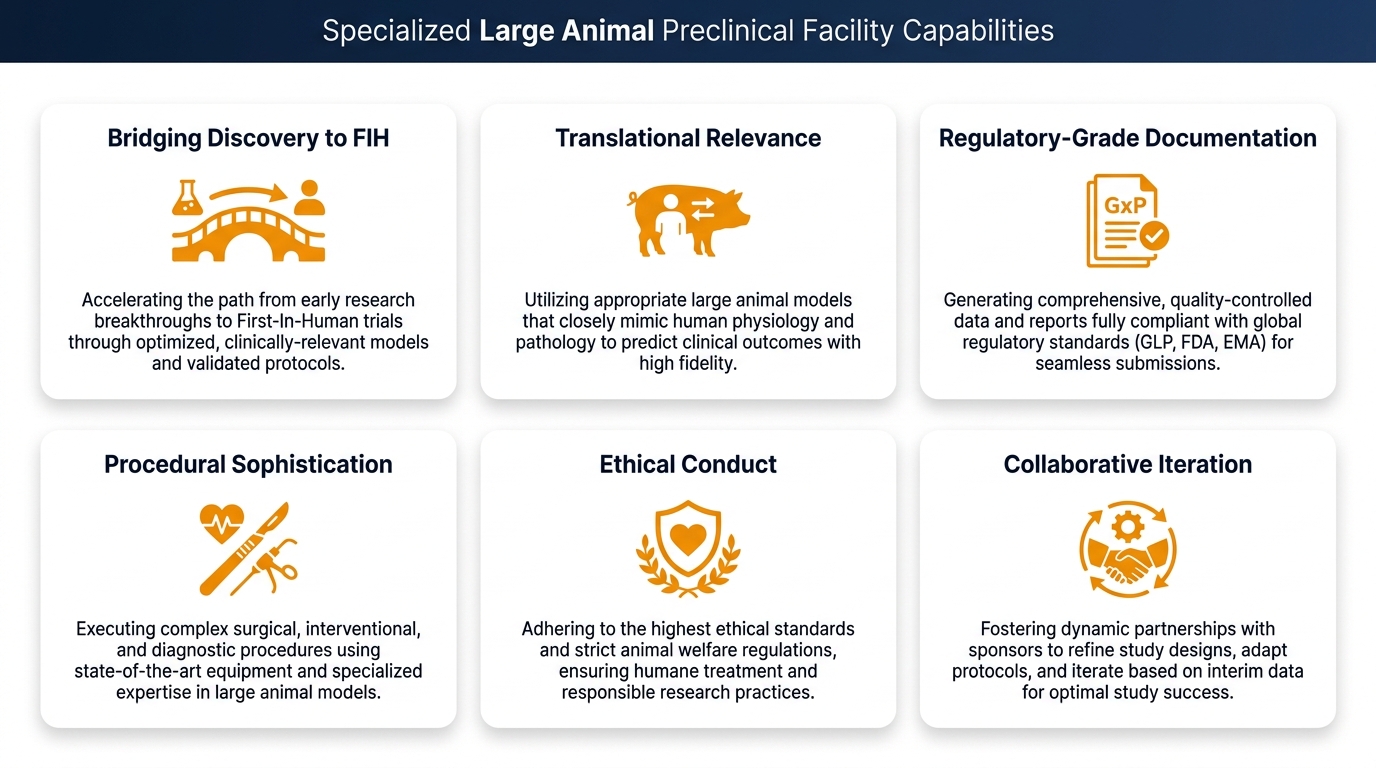
Many candidates — particularly medical devices, combination products, and certain biologics — require large animal models to generate IND-enabling and NDA-supportive data. The right facility brings together state-of-the-art surgical capabilities, scientifically supportive project management, and well documented procedures aligned with regulatory expectations.
| Sponsor Need | How a Tailored Preclinical Facility Supports It |
|---|---|
| Bridging discovery to FIH safely | Integrated IND-enabling study design with scientific escort throughout |
| Translational relevance | Large animal models (pig, sheep, rabbit) with humanoid-comparable anatomy |
| Regulatory-grade documentation | Structured reports suitable for nonclinical sections of IND/NDA dossiers |
| Procedural sophistication | Surgery rooms equipped with C-Arm fluoroscopy, high-definition ultrasound, and 4K laparoscopic towers |
| Ethical conduct | Animal welfare and 3Rs (Replacement, Reduction, Refining) embedded in every protocol |
| Collaborative iteration | Interactive conference space where sponsors and senior surgeons brainstorm protocol refinements |
“Continuity between IND-enabling and NDA-stage studies is not just convenient — it is a strategic advantage. A facility that generated your IND data already understands the candidate’s nonclinical fingerprint and can design the subsequent chronic toxicology and device performance studies with fewer surprises.”
— Adir Koreh, CEO, Biotech Farm Ltd. | 20+ Years Large Animal Model Expertise
Frequently Asked Questions
Ready to Map Your Preclinical Strategy from IND to NDA?
Are your IND-enabling studies aligned with the longer-term NDA expectations for your candidate — or are there gaps that could surface as a clinical hold or label restriction later? Building the right nonclinical program from the start saves time, capital, and regulatory friction.

This article is intended for informational purposes and reflects general regulatory principles. Sponsors should consult with qualified regulatory affairs professionals and review current FDA guidance documents for their specific development programs. References to ICH guidelines and CFR regulations are provided for directional context.