Preclinical Testing Medical Devices: A Comprehensive Guide to Safety, Models, and Regulatory Success
Bringing a medical device from concept to clinical use is a rigorous journey, and preclinical testing stands as the critical gateway between the laboratory bench and human application. For companies developing implantable, interventional, or tissue-contacting devices, understanding how preclinical testing works—and how to execute it effectively—can mean the difference between regulatory approval and costly delays.
Expert Insight: With over 30 years of combined expertise in preclinical research leadership, our team has guided hundreds of medical device programs through the complex pathway from bench testing to regulatory submission. The principles outlined in this guide reflect hard-won lessons from real-world device evaluations across cardiovascular, orthopedic, and interventional specialties.
What Exactly Is Preclinical Testing for Medical Devices?
Preclinical testing for medical devices refers to a structured series of evaluations conducted before a device enters human clinical trials or is submitted for regulatory clearance. These evaluations are designed to demonstrate that a device is safe and performs as intended when used as described in its labeling. The scope of medical device preclinical studies varies widely depending on the device type: a simple external bandage requires fundamentally different testing than an implantable cardiac stent.
The testing portfolio typically includes bench performance testing, material characterization, biocompatibility assessment, functional evaluation under simulated conditions, and—for many higher-risk devices—implantation or deployment in appropriate animal models. The FDA guidance on non-clinical bench performance testing outlines the expected content and format for these submissions, setting a clear benchmark for what data regulators want to see.
The Two Fundamental Questions
The overarching goal of preclinical device evaluation is to answer two fundamental questions:
- Does the device interact safely with biological tissue?
- Does it function reliably under realistic physiological conditions?
Only when both questions receive data-driven answers can a development program move confidently toward human trials.
Why Conduct Preclinical Testing Before a Clinical Trial?
The reasoning behind preclinical testing is straightforward but often underappreciated until a problem surfaces. At its core, the purpose is to reduce patient risk. A device that fractures under mechanical load, generates unexpected heat, or triggers an adverse tissue response must be identified and corrected long before it contacts a human patient.
Beyond patient safety, preclinical testing generates the foundational data that engineers, regulatory professionals, and clinical investigators rely on. It defines measurable endpoints—such as tissue integration rate, complication frequency, or device migration—that will later guide clinical trial protocols. Regulators expect this preclinical evidence to demonstrate that a clinical trial can be conducted with acceptable risk.
Key Benefit: Early identification of material fatigue, leakage, corrosion, or wear through bench and in vivo testing directly feeds back into design improvements—saving months of development time and potentially millions in failed clinical trials.
Does Every Medical Device Require Animal Testing?
Not necessarily. Medical device animal testing is not a universal requirement. The decision depends on several interrelated factors: the device’s classification and risk level, the nature and duration of body contact, the novelty of the technology, and whether adequate scientific alternatives exist.
The FDA’s guidance on animal welfare in testing emphasizes the 3Rs principle—Replacement, Reduction, and Refinement—as a guiding framework for determining when animal studies are truly necessary.
For simpler, non-invasive, or well-characterized devices, bench testing combined with in vitro assays and risk analysis may suffice. However, for complex medical devices requiring direct interaction with living systems, a thorough understanding from preclinical studies on animals often serves as the bedrock for moving forward.
When There Is No Reliable Alternative to In Vivo Testing
Certain aspects of device performance simply cannot be replicated outside a living organism:
- Evaluating thrombogenicity in the presence of flowing blood
- Assessing chronic tissue healing and integration around an implant
- Monitoring immune response over weeks or months
- Observing device behavior in a dynamic physiological environment
Comparing In Vitro, In Vivo, and In Silico Approaches
Three distinct methodological categories form the toolkit of preclinical device evaluation, and understanding their respective roles prevents both over-testing and under-testing.
| Approach | Definition | Typical Use | Limitations |
|---|---|---|---|
| In Vitro | Testing in controlled lab environments using cells, tissues, or simulated body fluids | Biocompatibility screening, corrosion testing, cytotoxicity | Cannot replicate systemic physiological responses |
| In Silico | Computational modeling and simulation using digital tools | Stress analysis, fatigue prediction, fluid dynamics | Dependent on model accuracy; regulatory acceptance evolving |
| In Vivo | Testing in live animal models under controlled conditions | Implant integration, chronic safety, functional performance | Higher cost and time; ethical considerations |
The typical workflow begins with bench and in vitro testing for initial design screening, progresses through in silico modeling for optimization, and culminates in targeted in vivo studies only when the previous stages confirm the design is mature enough.
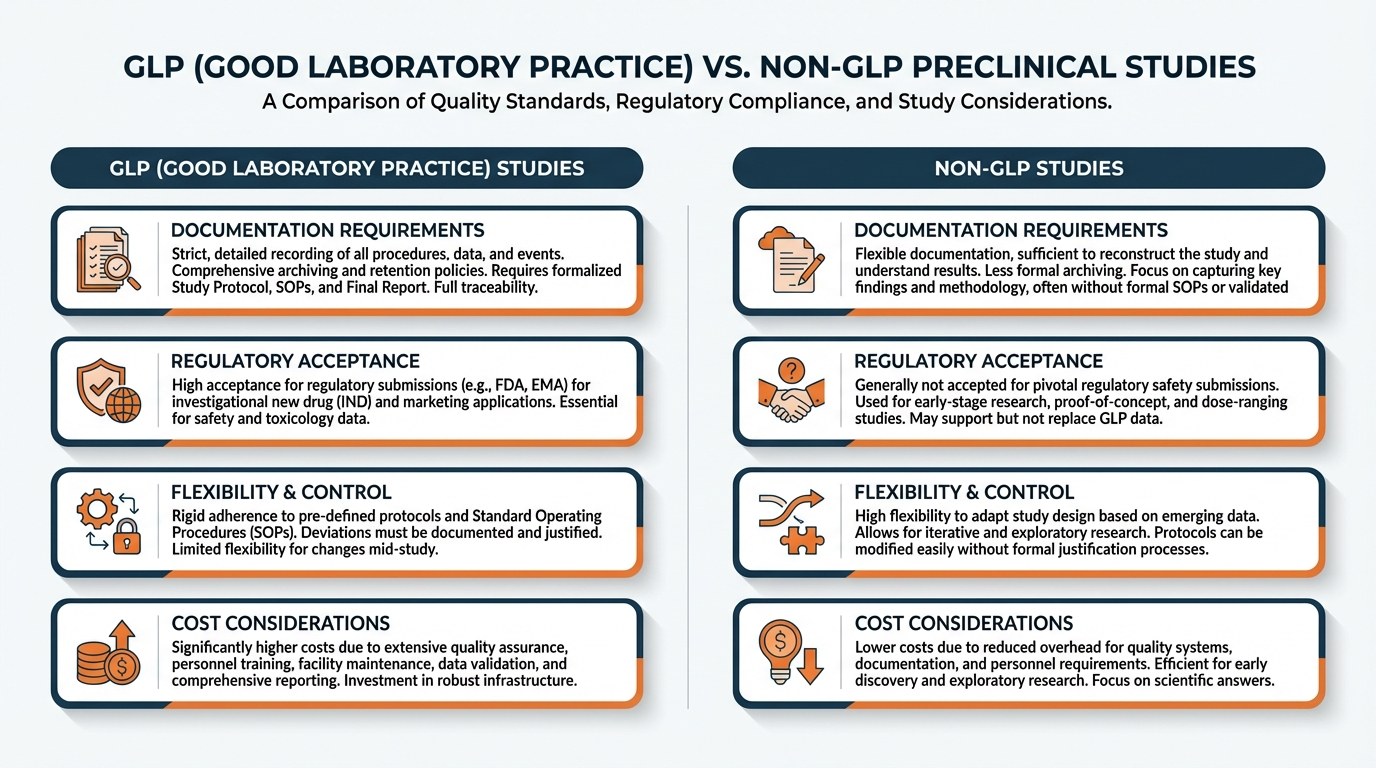
GLP vs. Non-GLP Preclinical Studies: What Is the Difference?
Good Laboratory Practice (GLP), as codified in 21 CFR Part 58, establishes stringent standards for the planning, conduct, monitoring, recording, and reporting of non-clinical laboratory studies. GLP is not about the science itself—it is about the integrity, traceability, and auditability of the data generated.
Understanding the nuances of GLP animal studies is crucial for ensuring the integrity and acceptance of your data by regulatory bodies.
When Non-GLP Is Appropriate
- Early-stage feasibility work
- Proof-of-concept evaluations
- Iterative design comparisons
- Surgical technique development
When GLP Is Required
- IDE application support
- 510(k) or PMA submissions
- CE marking technical files
- Any formal regulatory submission
The OECD Principles on Good Laboratory Practice reinforce this internationally, describing GLP as a managerial and procedural framework that ensures reliability and reproducibility of reported findings.
Which Device Types Typically Require In Vivo Research?

The need for medical device animal testing correlates directly with device complexity, invasiveness, and risk classification. The following categories almost universally require in vivo evaluation:
Implantable Devices
Pacemakers, stents, joint replacements, spinal fusion hardware. For example, the development of an Orthopedic Medical Device almost always necessitates in vivo research to assess bone integration and load bearing.
Vascular & Cardiac Devices
Must demonstrate performance in flowing blood, under cardiac motion, and in the presence of endothelial tissue.
Energy-Delivering Devices
Devices applying radiofrequency, laser, ultrasound, or cryogenic energy require in vivo studies to characterize thermal or ablative effects.
Tissue-Interacting Devices
Wound dressings with active biological components, drug-device combinations, and tissue scaffolds.
Ultimately, comprehensive preclinical evaluation culminates in robust safety and efficacy studies demonstrating the device’s performance in conditions that closely approximate clinical reality.
How to Select the Right Animal Model for Device Safety Testing
Choosing the appropriate species and model is one of the most consequential decisions in preclinical device evaluation. The selection must be driven by anatomical and physiological relevance to the human target site—not by habit, convenience, or cost alone.
Key Selection Considerations
- Vessel diameter and organ size
- Bone density and healing rate
- Tissue elasticity and hemodynamic parameters
- Feasibility of performing the intended surgical procedure
- Imaging equipment availability (fluoroscopy, echocardiography, OCT)
Choosing appropriate animal models for preclinical research is a critical step in ensuring the relevance and applicability of study results to human physiology. Biotech Farm’s state-of-the-art facility is specifically equipped for large animal models—pigs, sheep, goats, and calves—that are physiologically similar to humans in key organ systems.
⚠️ Common Mistakes in Model Selection
The FDA’s guidance on animal studies for medical devices highlights several pitfalls:
- Selecting a model based solely on lower per-animal cost
- Ignoring the primary endpoint (e.g., species with different healing biology)
- Size mismatches preventing proper device deployment
- Underestimating follow-up duration for chronic performance data
What Endpoints Are Measured in Animal Testing for Medical Devices?

Endpoints in preclinical device evaluation fall into three broad categories: safety, performance, and handling. The specific endpoints selected must align directly with the device’s intended use and the claims the manufacturer intends to make.
| Endpoint Category | Examples | Measurement Methods |
|---|---|---|
| Safety | Tissue inflammation, fibrous capsule thickness, thrombosis rate, infection incidence | Histopathology, blood panels, gross necropsy, imaging |
| Performance | Lumen patency, implant integration, mechanical stability, energy delivery accuracy | Angiography, micro-CT, biomechanical pull-out testing, thermal mapping |
| Handling | Deployment success rate, procedural duration, ease of positioning | Procedural video documentation, operator scoring, fluoroscopy records |
A mismatch between study endpoints and regulatory questions is one of the most common reasons for deficiency letters from reviewing agencies.
— FDA Review Experience
How Long Does Preclinical Testing Take?
Timelines vary enormously based on study complexity and regulatory requirements:
| Study Type | Typical Timeline | Key Variables |
|---|---|---|
| Bench-only testing (low-risk device) | 4-8 weeks | Number of tests, complexity |
| Non-GLP feasibility (acute/30-day) | 2-4 months | Animal availability, pathology processing |
| Full GLP study (chronic follow-up) | 6-18 months | Protocol prep, ethical approvals, follow-up duration |
Timeline Tip: Pathology—especially histology of implant sites requiring hard-tissue processing—is frequently the longest single component, sometimes adding 2-3 months. Working with a partner like Biotech Farm, which maintains dedicated surgical suites with C-arm fluoroscopy, high-definition ultrasound, and laparoscopic equipment on-site, eliminates scheduling bottlenecks that can delay programs at less specialized centers.
What Determines the Cost?
Cost is best understood as a composite of discrete components:
- Procedural complexity: Open surgery vs. catheter-based intervention
- Number of animals and groups: Multiplies per-subject expenses
- Follow-up duration: Affects housing, veterinary care, monitoring
- Laboratory analyses and pathology: Blood chemistry, histology, special stains
- GLP requirements: Quality assurance overhead, audit costs
Reducing the Risk of Failure in Preclinical Testing
Failures in preclinical studies are rarely random—they usually trace back to preventable causes. The most effective risk-reduction strategy is conducting early non-GLP iterations before committing to a formal GLP study.
Common Failure Modes to Prevent
- Mid-study design changes that invalidate earlier data
- Inconsistent device manufacturing introducing variability
- Selection of non-measurable or irrelevant endpoints
- Choosing an animal model that doesn’t represent target anatomy
Red Flags Before Launching a GLP Study
Warning Signs Your Program Isn’t Ready:
- Device design still changing between prototype iterations
- Insufficient bench or in vitro data
- Unclear regulatory pathway (510(k) vs. PMA vs. CE marking)
- Budget constraints forcing compromises on group size or follow-up duration
Essential Deliverables from Every Preclinical Project
Regardless of study scope or regulatory pathway, certain deliverables should be standard. Facilities like Biotech Farm, with over 30 years of experience managing preclinical research on large animals, understand that meticulous documentation is as important as the science itself.
???? Approved Protocol
Signed before the study begins, establishing the rules of engagement.
???? Raw Data
Maintained in unaltered form, providing the evidentiary foundation.
???? Deviation Log
Captures any departures from protocol with justification and impact assessment.
✅ QA Statements
Confirm independent review for GLP compliance.
???? Final Report
Synthesizes all findings in regulatory-aligned format.
????️ Archived Imaging
Original files (fluoroscopy, ultrasound, micro-CT) accessible for review.
Frequently Asked Questions
Ready to Plan Your Device’s Preclinical Pathway?
Whether you are developing a novel implant, refining an interventional tool, or preparing a regulatory submission for a tissue-contacting device, the quality of your preclinical program shapes everything that follows. What questions does your device still need to answer before it can safely reach a patient?
If you are ready to discuss study design, model selection, or GLP requirements with a team that brings decades of hands-on experience in large animal preclinical research, we’re here to help.