Expert Preclinical Research Guidance
Preclinical Study Endpoints: The Complete Expert Guide to Selection, Design & Regulatory Alignment
With over 20 years of hands-on large-animal model expertise and a multidisciplinary team of seasoned veterinarians who have worked together for more than a decade, BIOTECH FARM Ltd. has guided hundreds of preclinical programs — from first-in-animal feasibility studies to full GLP IND-enabling packages. The single most common factor in failed or inconclusive preclinical studies is not the intervention itself: it is a poorly constructed endpoint architecture. This guide presents the definitive, expert-level framework for selecting, justifying, and executing preclinical study endpoints that withstand regulatory scrutiny and generate genuinely translatable data.
🔎 Expert Insight
The most expensive mistake in preclinical research is not a failed compound — it is a failed study design. When endpoints are vague, mismatched to the model, or defined post-hoc, even a genuinely active drug or device can produce uninterpretable data. Investing in rigorous endpoint architecture before a single animal is enrolled protects your timeline, your budget, and ultimately the regulatory credibility of your entire development program.
What Are Preclinical Study Endpoints and Why Are They Critical for Research Success?
Preclinical study endpoints are the predetermined, measurable outcomes used to evaluate the safety, efficacy, or mechanism of action of a candidate drug, biologic, or medical device in non-human biological systems. They function as the scientific compass of any nonclinical investigation, translating an abstract hypothesis into quantifiable variables that determine whether a study succeeded or failed.
A robust endpoint must be measurable, sensitive to biological change, reproducible across cohorts, and tightly linked to the underlying research question. When endpoints are vague, redundant, or weakly justified, even a genuine pharmacological effect can be masked by noise — producing inconclusive datasets that delay regulatory submission and waste animal resources. Well-designed studies with clearly articulated endpoints are essential for generating interpretable, defensible data that can support downstream IND submissions and translational decisions.
How Do You Choose a Primary Endpoint in an Animal Study?
The primary endpoint is the single, most important measurable outcome that directly addresses the central research question. It is the variable that drives sample size calculations, governs the statistical analysis plan, and ultimately determines whether the study confirms or refutes the working hypothesis. Selecting a primary endpoint demands disciplined alignment between the study aim, the biology of the disease model, and the regulatory pathway.
The endpoint must be defined unambiguously before the first animal is enrolled, with explicit thresholds for what constitutes a positive or negative result. Choosing a primary endpoint is integral to successful IND-enabling study design, where a misaligned primary measure can derail an entire development program.
How to Ensure the Primary Endpoint Truly Answers the Research Question
A defensible primary endpoint must have a direct, causal link to the hypothesis rather than a merely correlational association. It should exhibit relatively low intrinsic variability within the chosen experimental system, so that biological effects are not drowned by background noise. Finally, it requires a standardized, rigorously documented measurement protocol — including instrument calibration, blinding procedures, and pre-specified scoring rubrics — to ensure consistency across operators, time points, and replicate cohorts.
Direct Causal Link
The endpoint must directly test the hypothesis, not a downstream correlate that may or may not track the mechanism of interest.
Low Intrinsic Variability
Biological signal must exceed background noise within the experimental system to produce interpretable results with feasible sample sizes.
Standardized Protocol
Calibrated instruments, operator blinding, and pre-specified scoring rubrics ensure reproducibility across cohorts and time points.
Primary, Secondary, and Exploratory Endpoints: Drawing the Line
Distinguishing between endpoint tiers prevents data dredging and protects statistical integrity. Primary endpoints carry the main hypothesis and the inferential weight of the study. Secondary endpoints provide supporting context — mechanistic readouts, pharmacodynamic markers, or broader physiological effects — but they are not powered for confirmatory hypothesis testing. Exploratory endpoints are intentionally hypothesis-generating, intended to surface signals worth pursuing in follow-up work.
Inflating the number of endpoints without multiplicity adjustments inflates Type I error and produces apparent “wins” that do not replicate. A disciplined hierarchy keeps the statistical analysis plan honest.
| Endpoint Tier | Statistical Role | Typical Example |
|---|---|---|
| Primary | Powered for hypothesis testing; drives conclusion | Reduction in infarct size at 28 days |
| Secondary | Supportive context; not confirmatory | Plasma biomarker kinetics |
| Exploratory | Hypothesis-generating; descriptive | Transcriptomic signatures in target tissue |
What Are Efficacy Endpoints in Preclinical Studies and How Is “Efficacy” Defined Without Clinical Results?

Efficacy endpoints in preclinical research are functional or biological measures showing that an intervention consistently alters disease pathology or phenotype in a relevant animal model, indicating a plausible therapeutic benefit. Without human clinical outcomes available, “efficacy” is operationalized through model-specific readouts: reduction in tumor volume, improvement in locomotor scores, normalization of glycemic curves, or modulation of mechanistically anchored biomarkers.
The chosen efficacy endpoint must be biologically tied to both the disease model and the candidate’s mechanism of action — measuring an irrelevant downstream marker, however convenient, undermines translational value.
Quick Example of a Good Efficacy Endpoint Set
✅ The Three-Layer Efficacy Architecture
- Functional endpoint: Behavioral, physiological, or performance-based measure reflecting real-world impact.
- Structural endpoint: Histology, MRI, micro-CT, or anatomical imaging confirming pathological change.
- Mechanistic PD biomarker: Target engagement and pathway modulation confirmation to validate the mechanism.
Scenario: Safety Endpoints in Animal Models and Early Risk Identification
Imagine a novel small molecule entering its first GLP repeat-dose study. Safety endpoints function as the early warning system that detects adverse effects before they become dose-limiting in humans. A comprehensive battery typically includes gross clinical observations, body weight, food consumption, hematology, clinical chemistry, urinalysis, organ weights, and full histopathological examination of target and incidental tissues.
These measures collectively define the No Observed Adverse Effect Level (NOAEL) and inform exposure margins for the IND. For biologics, the safety endpoint matrix is broader and often includes immunogenicity, cytokine release, and complement activation — examined in depth within preclinical packages for biologics.
⚠️ Critical Safety Note
Safety endpoints must be defined before the study begins and should include pre-specified criteria for what constitutes a toxicological signal. Discovering a safety parameter post-hoc — or adding endpoints during the study — invalidates the GLP integrity of the data and may require full study repetition.
Nonclinical Versus Clinical Endpoints: Where the Line Sits
Nonclinical endpoints are biological, laboratory, or pathological measurements collected in in vitro or in vivo preclinical studies. Clinical endpoints, by contrast, reflect how a human patient feels, functions, or survives — symptom relief, disease-free interval, overall survival.
Nonclinical endpoints are prized for their sensitivity, speed, and granularity, but their translational value depends entirely on the strength of the scientific justification linking them to eventual clinical benefit. A histological improvement in a rodent model does not automatically forecast a patient-reported outcome; the bridge must be argued and, ideally, supported by mechanistic evidence and cross-species comparability data.
“A preclinical endpoint is only as valuable as the scientific argument connecting it to a clinically meaningful outcome. The measurement itself is never sufficient — the translational bridge must be built and defended.”
— BIOTECH FARM Ltd. Scientific Team
When Is a Biomarker an Endpoint, and When Is It Just Supportive?
A biomarker rises to the status of an endpoint when it is prospectively defined in the protocol, reliably and reproducibly measurable, and convincingly tied to a meaningful change in disease state. If any of those conditions is missing, the biomarker remains a secondary or exploratory readout — informative, but not confirmatory.
Regulatory authorities draw a sharp line between clinical outcomes and surrogate endpoints, and they expect robust analytical and biological validation before accepting a biomarker as a substitute for a true outcome measure. Documentation, assay qualification, and pre-specified acceptance criteria are non-negotiable.
✅ Biomarker AS Endpoint (When All 3 Met)
- Prospectively defined in the protocol
- Reliably and reproducibly measurable
- Convincingly tied to meaningful disease state change
🔴 Biomarker as Supportive Only (Any Condition Missing)
- Added after study initiation (post-hoc)
- Assay not formally qualified or validated
- Biological link to disease outcome unestablished
Surrogate Endpoints: Useful Shortcut or Hidden Trap?
A surrogate endpoint is a measurable marker intended to substitute for a clinical outcome endpoint. It becomes hazardous when improvement in the surrogate does not faithfully predict improvement in the underlying clinical outcome. A classic illustration: tumor shrinkage is easier to measure than overall survival, yet the two are not always correlated, and interventions that shrink tumors transiently may not extend life.
The accepted standard requires demonstrated, quantitative evidence that changes in the surrogate reliably forecast the clinical endpoint of interest. Understanding surrogate endpoints is also central to implant safety studies, where inflammation markers and tissue-integration scores stand in for long-term device performance.
🚀 When Surrogate Endpoints Work Well
Surrogate endpoints deliver genuine value when: (1) there is a biologically plausible and mechanistically supported pathway from surrogate to clinical outcome; (2) prior trials have established a quantitative correlation; and (3) the surrogate can be measured with validated, standardized assays. In these circumstances, surrogates accelerate development timelines without sacrificing scientific integrity.
Common Mistake: Matching Endpoints to the Wrong Animal Model
One of the most expensive errors in preclinical research is selecting endpoints based on what is easy to measure rather than what the animal model actually recapitulates. If a model does not reliably express the target phenotype — functional deficit, pain behavior, progressive pathology — then a functional endpoint built around that phenotype will be unstable, noisy, or simply irrelevant.
The species, strain, induction protocol, and time course must all align with the chosen readout. This principle is critical in endoscopic device testing animals, where anatomical realism dictates which endpoints are even meaningful. It applies equally to drug delivery systems preclinical testing, where route, kinetics, and tissue distribution must match the endpoint architecture.
📝 Case Study: Anatomical Realism in Large-Animal Endoscopy Models
A medical device sponsor attempted to evaluate a novel endoscopic deployment system in a rodent model, measuring deployment accuracy as the primary endpoint. The gastrointestinal anatomy of rodents is fundamentally incompatible with human-scale devices, producing endpoint data that was mechanically irrelevant and biologically uninterpretable.
Resolution: Transitioning to a porcine model with humanoid-organ scale anatomy aligned the endpoint to the clinical use case, generated valid deployment accuracy data, and enabled a direct path to regulatory submission. The model and the endpoint must be co-designed — neither can be selected in isolation.
How a Humane Endpoint Is Defined in Animal Studies
A humane endpoint is the earliest scientifically justifiable point at which an animal experiencing pain, distress, or suffering is relieved from that state — typically through euthanasia — without compromising the integrity of the data collected up to that moment. Humane endpoints are protocol-level commitments, predefined and reviewed by an institutional ethics committee (IACUC or its national equivalent), and based on observable clinical signs, physiological thresholds, or quantifiable indicators such as body weight loss, tumor burden, or behavioral non-responsiveness.
They embody the practical application of the 3Rs — Replacement, Reduction, and Refinement — and are anchored in Israel by the framework of the Council for Animal Experimentation and institutional ethics committees at academic centers.
Replace
Substitute in vivo studies with in vitro or computational methods wherever scientifically justified.
Reduce
Use minimum animal numbers consistent with adequate statistical power and reliable endpoint measurement.
Refine
Employ humane endpoints and the best available techniques to minimize pain, distress, and suffering throughout.
How Endpoints Shape Sample Size and Statistical Power
The primary endpoint determines the sample size required to detect a biologically meaningful effect with adequate power — usually 80% or higher — at a pre-specified significance level. Each additional primary or co-primary endpoint introduces multiplicity, which must be controlled using methods such as Bonferroni, Holm, or hierarchical testing.
Effect size assumptions, variability estimates from pilot data, and expected attrition all feed into the calculation. Underpowered studies waste animals and yield ambiguous results; overpowered studies waste resources and raise ethical concerns. The endpoint and the sample size are inseparable design decisions.
💡 Sample Size Calculation: Key Inputs
- Effect size: The minimum biologically meaningful difference you need to detect.
- Variability: Standard deviation from pilot or historical data in your specific model.
- Alpha (significance level): Typically 0.05; adjust for multiplicity if co-primary endpoints are used.
- Power: 80% minimum; 90% preferred for pivotal IND-enabling studies.
- Attrition: Add 10–20% to account for animal losses, exclusions, and technical failures.
Typical Endpoints in GLP Toxicology Studies
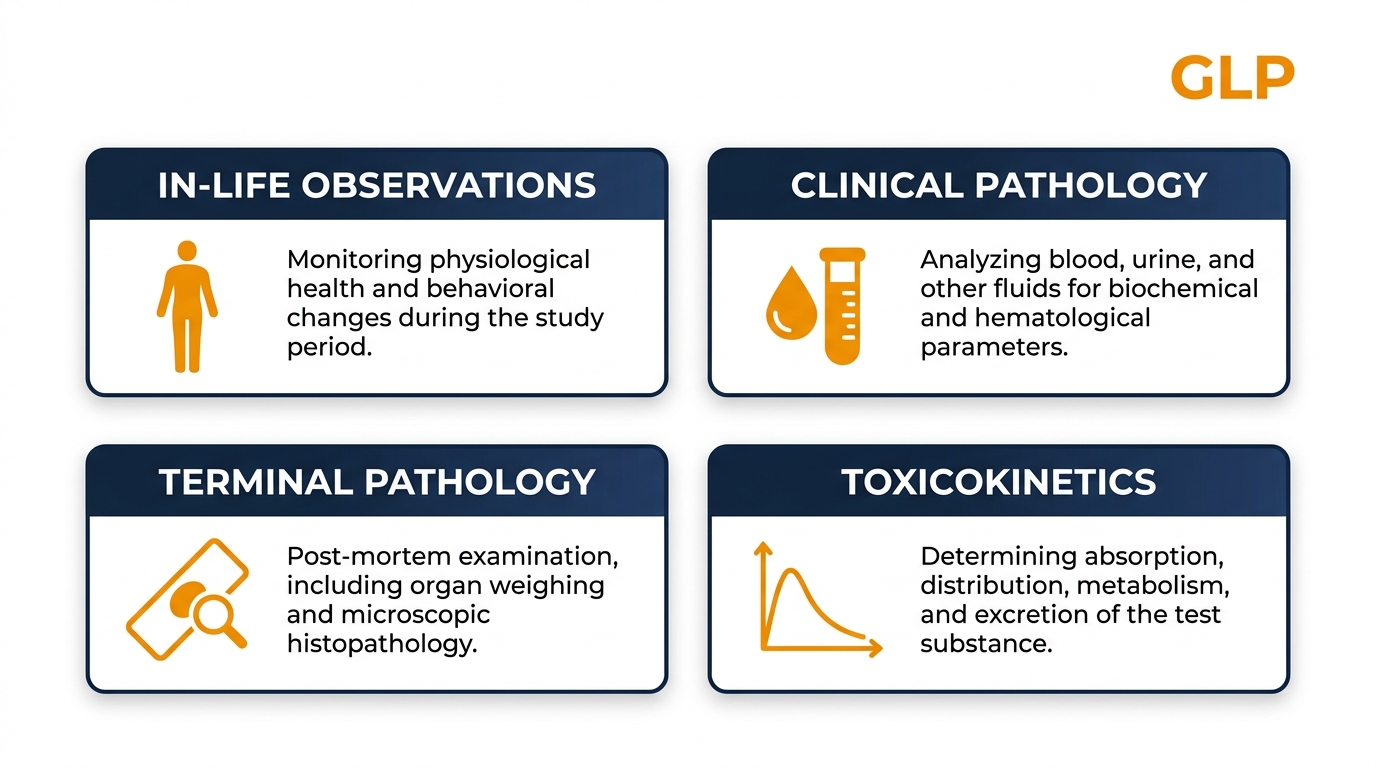
GLP toxicology studies follow a standardized endpoint architecture designed to expose any systemic or organ-specific toxicity within a defined exposure window. The core battery is consistent across most regulatory frameworks and covers four principal domains:
| Category | Representative Endpoints | Purpose |
|---|---|---|
| In-life observations | Clinical signs, body weight, food consumption | Detect overt toxicity and well-being changes |
| Clinical pathology | Hematology, clinical chemistry, urinalysis, coagulation | Identify organ stress and systemic effects |
| Terminal pathology | Organ weights, gross necropsy, histopathology | Characterize target organs of toxicity |
| Toxicokinetics | Plasma exposure, AUC, Cmax | Link exposure to observed effects |
How the BIOTECH FARM Platform Supports Endpoint-Driven Design
Endpoint selection is only as strong as the operational platform that executes it. Working in a large-animal facility built around humanoid-organ relevance — pig, sheep, rabbit, and goat models — enables endpoints in cardiology, ophthalmology, orthopedics, and respiratory research that small-rodent platforms simply cannot deliver.
Integrated imaging suites — C-Arm fluoroscopy, high-definition ultrasound, echocardiography, OCT, 4K laparoscopic towers — allow structural and functional endpoints to be captured under realistic surgical conditions. Scientific escort through protocol design, ethics submission, and execution helps sponsors translate a research question into a measurable, defensible endpoint set without losing months in iteration.
| Sponsor Need | How the Platform Supports It |
|---|---|
| Translational relevance | Large-animal models with humanoid-organ anatomy (pig, sheep, rabbit, goat) |
| Structural endpoints | Integrated fluoroscopy, high-definition ultrasound, OCT, echocardiography, microscopy |
| Regulatory-grade documentation | Well-documented procedures aligned with GLP expectations and regulatory frameworks |
| Ethical endpoint design | Pre-approved humane endpoints under IACUC-equivalent ethics committee oversight |
| Protocol refinement | Scientific escort and brainstorming with experienced surgeons and veterinarians |
“Our team does not simply run experiments — we co-design the scientific question. By aligning the animal model, the endpoint architecture, and the regulatory context before a single animal enters the facility, we dramatically increase the probability that the data generated will be interpretable, translatable, and accepted by the relevant authority.”
— Adir Koreh, CEO, BIOTECH FARM Ltd.
Final Checklist for Endpoint Selection
🎯 Is Your Endpoint Relevant?
Does it address a specific biological or disease question tied to your hypothesis? Is the readout meaningful in the context of the human condition you ultimately intend to treat? An endpoint disconnected from clinical reality will produce data that cannot be translated, regardless of how clean the statistics look.
📏 Is Your Endpoint Measurable and Reliable?
Can it be quantified accurately, consistently, and with low inter- and intra-observer variability? Reliable measurement methods — calibrated instruments, blinded scoring, validated assays — are crucial for endpoint validity.
🔬 Is Your Endpoint Sensitive and Specific?
Can it detect changes caused by your intervention without being confounded by extraneous factors such as handling stress, circadian variation, or dietary fluctuation? Is it specific to the mechanism of action under investigation?
⚖️ Is It Ethical and Compliant?
Does the endpoint minimize unnecessary suffering through well-defined humane endpoints? Does it align with national and international animal welfare regulations, including principles from the Israeli Council for Animal Experimentation?
Frequently Asked Questions
Ready to Define Endpoints That Hold Up Under Regulatory Scrutiny?
Whether you are scoping a first-in-animal study, preparing an IND-enabling package, or refining a complex device protocol — our team can help you map the scientific question to a measurable, ethically sound, and statistically defensible endpoint architecture in a large-animal setting.